On Vaccination in Ireland
Following from my weekend post about issues with Covid19 vaccination, which seems to have ruffled a few feathers, I thought I’d just mention a couple of recent developments.
The first is that on Tuesday (yesterday) the Irish Government decided to change the way it vaccinates the rest of the population. The previous plan was rather complicated with a number of groups to be vaccinated in order of priority:
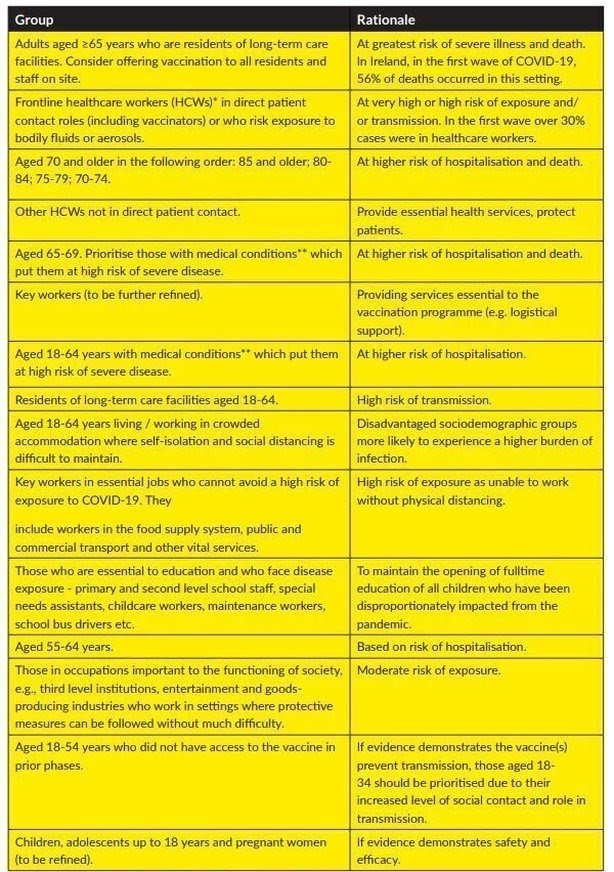
That plan has now been scrapped and after the current groups 1-3 are completed it will revert to a simpler scheme with priority determined only by age. As an oldie I will benefit from this, moving up several steps in the pecking order as a consequence of the decision.
Frontline workers such as teachers and Gardaí are dismayed by this decision. On the news just now various folk were trying to argue that the change is for health policy reasons, stating that the prime factor in risk for Covid-19 is age. Actually, it isn’t. The prime factor is exposure to the virus.
What I mean is that the probability of dying from Covid-19 if you haven’t been infected is zero: 100% of those suffering death or serious illness from Covid-19 have been in contact with the virus. Someone who is 60 years old but able to work effectively at home at far lower risk of exposure than a 35 year old schoolteacher.
The real reason for the change is that Ireland does not possess a system that can be used identify groups by occupation in an efficient way. Doing it by age is far simpler and would lead to a much more rapid rise in the fraction of the population immunized. Sometimes decisions have to be made for such practical reasons, but I do wish certain people were more honest.
The slow rollout of the vaccine in Ireland should have provided the Government to work out how to implement their original strategy. Obviously they decided that they couldn’t.
Anyway, for myself, I am pleased that it now looks quite likely that I’ll get at least one jab by May. Assuming the vaccine supply holds up, of course.
I thought I’d end with a thought following on from my earlier post. Some people will ask whether I would have the AstraZeneca vaccine given my views about the company’s behaviour and the lower efficacy of the vaccine as compared to others available.
I think there are two motivations for getting vaccinated. One is self-preservation. I want to protect myself as much as possible. If I had the choice of vaccine for this reason I would pick Moderna or Pfizer-BioNtech but would accept AZ if that was the only one available. As things stand, over 75% of doses administered in Ireland have been Pfizer-BioNtech,
The other motivation is to help reduce the transmission of the disease. For that even a low efficacy vaccine would play a part. If the only shot available offered just 50% protection I would still take it, as if everyone did so the population dynamics would still be significantly slowed.
It’s a similar thing with face masks, actually. Their role is only partly to protect the wearer. The other part is to protect everyone else.
So on both grounds, yes I would take the AZ vaccine if that was the only one on offer, but if I had the choice I would pick a better one. I feel the same way about the Johnson & Johnson vaccine, which will start to become available in Ireland very soon.
Follow @telescoper
March 31, 2021 at 7:11 pm
Yes, that is a concern but they are very rare events so I think I’d be prepared to take the risk.
March 31, 2021 at 7:34 pm
Based on the numbers I saw (which may have been updated since) the rate of thrombosis among vaccine recipients of AZ was actually LOWER than the comparable rate of thrombosis in the general population. That was a rough estimate, but still…doesn’t seem to be a statistically significant effect. It’s a bit like when one looks at the package insert of a pharmaceutical and sees one of the reported side-effects is “upper respiratory infection”.
March 31, 2021 at 8:39 pm
That was the risk of thrombosis in general. The concern is not about that (although there was some initial concern) but about the very specific and rare cerebral vein thrombosis with low platelet count (and possibly some other similar cases).
April 1, 2021 at 2:36 pm
Thank you! I wasn’t aware of those more specific concerns.
April 1, 2021 at 11:22 am
Healthcare staff are overwhelmingly female and under 55. 2 out of the 62 cases reported in EU/EEA as of yesterday were men, which appears to be fewer than you would expect even assuming all were healthcare staff. There is as yet no clear evidence pointing to any other distinguishing factors. Women over 50 do not take contraceptives.
For the record, i would take the AZ vaccine if offered it.
April 1, 2021 at 2:38 pm
Hear hear. Where I am, I got the Pfizer one (first dose, so far), and only had local soreness, even though I’ve had the actual virus…which I do NOT want to have again!
April 1, 2021 at 2:37 pm
That IS interesting, and certainly seems pertinent.
March 31, 2021 at 9:38 pm
Striking contrast between headlines in Irish Times and on the NRK (norwegian broadcasting) website.
Irish Times: “No evidence for restricting AstraZeneca use, says European Medicines Agency”
NRK: “The [Norwegian] Medicines Agency: Serious with 62 cases in Europe”
Johnson&Johnson and Sputnik are similar vaccines (but using human rather chimp adenoviruses as vectors) so no doubt they will be watched closely. No evidence of such side effects from the mRNA vaccines.
March 31, 2021 at 9:48 pm
“various folk were trying to argue that the change is for health policy reasons, stating that the prime factor in risk for Covid-19 is age. Actually, it isn’t. The prime factor is exposure to the virus.”
I think you are mistaken here. My understanding is that the immunisation advisory committee has considered the total risk of severe illness, including exposure, and found that no occupational group apart from healthcare workers has any significantly higher risk of illness than others. The 60-year-old who is working from home may well be living with someone who is at high risk of infection, while the 35-year-old teacher is at very low risk of getting seriously ill even if she catches the virus. Actually, figures from Norway suggest that secondary school teachers are at lower risk of infection than the average population.
April 1, 2021 at 8:58 am
Don’t underestimate the risk of long covid. The death toll only tells half the story. The effects can linger for a long time.
April 1, 2021 at 11:11 am
P(D) = P(I)P(D|I).
The advisory committee evaluated the evidence regarding P(D), which is ultimately the meaningful measure, and also easier to determine than the two others. D here stands not just for death, but for severe disease (requiring hospitalisation).
Long Covid is an issue which is still poorly understood, but only a minority suffer from it. I do not think there is any evidence that younger people are at higher risk of it. The anecdotal evidence we hear is largely about younger people but that is because this is more newsworthy.
There is some intriguing anecdotal evidence that vaccination may cure long Covid. Way too early to say if this is real.
April 1, 2021 at 11:22 am
The LHS of your equation should be P(D, I).
April 1, 2021 at 11:24 am
True, but P(D)=P(D,I) since D => I.
April 1, 2021 at 1:51 pm
Strictly speaking 1 million UK residents is a minority but I wouldn’t call it ‘only a minority’. The highest prevalence rate is reported among 25-34 year olds. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/1april2021
April 1, 2021 at 3:39 pm
That is a very interesting article. It is also exemplary in stressing its caveats and limitations. Taking the self-reported 1.1m at face value, that would represent something like 1 in 10 of those who have been infected. The official number of cases in the UK is 4.5m but those are almost all second wave cases, and it is clear the first wave (where very little testing happened) was at least as large.
This tallies well with the 1 in 8 reported from the systematic study.
The prevalence is consistent in all age groups between 25 and 70.